
Executive Summary
Hypertension is the most prevalent and most modifiable cardiovascular risk factor in adult medicine. It is also one of the most poorly managed.
Roughly 120 million American adults have high blood pressure. Fewer than 60 percent are aware of the diagnosis. Only about 1 in 5 reach blood pressure control. The damage progresses for years, often decades, before any symptom appears.
In August 2025, a coalition led by the American Heart Association and the American College of Cardiology released the first major update to the hypertension guideline since 2017. It changed how risk is calculated, how diagnosis is confirmed, when treatment is initiated, and how lifestyle is prescribed.
This brief examines three areas where the gap between the new standard and ordinary clinical practice is largest. Each is also where HealthSpan Longevity Living is structurally designed to close it.
The diagnostic process must be more precise.
The treatment architecture must be more deliberate.
The lifestyle prescription must be treated as clinical, not optional.
Each is addressed in turn below.
Table of Contents

The Scope Of The Problem
Hypertension is rarely framed as urgent for any individual patient. It produces no symptoms in its silent decades. The arteries respond to elevated pressure thousands of times a day, year after year, without any warning to the person carrying them.
The aggregate consequences are well established. Hypertension is the leading preventable risk factor for heart attack, stroke, heart failure, kidney disease, cognitive decline, and dementia. It contributes substantially to the cardiovascular disease that accounted for over $400 billion in direct healthcare expenditures and lost productivity in 2020 to 2021.
Three statistics matter most for the audience of this brief.
In adults under age 40, 60 percent of those with hypertension do not know they have it.
Fewer than 60 percent of all American adults with hypertension are aware of the diagnosis.
Only about 1 in 5 reach blood pressure control.
These are not failures of patient effort. They are failures of system design. Hypertension is treated, in most settings, as a single number to be lowered to a single threshold. The biology is neither that simple nor that forgiving.
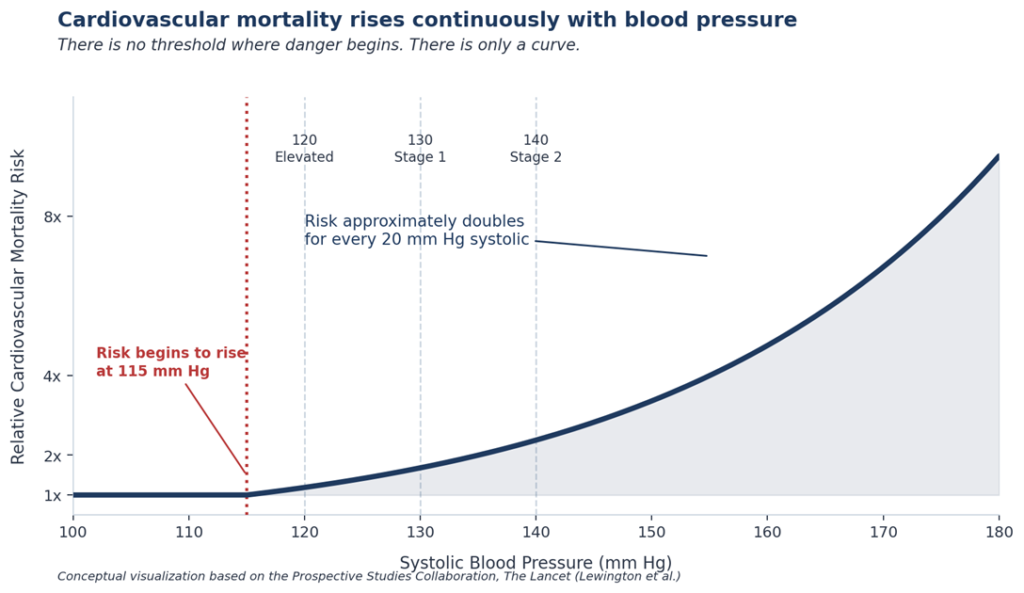
The largest analysis of blood pressure and cardiovascular risk ever conducted, covering nearly one million adults across 61 prospective studies, found that cardiovascular mortality begins climbing at a systolic pressure of 115 mm Hg. From that point upward, the risk roughly doubles for every 20 mm Hg of additional systolic pressure. The relationship is continuous and present across every age group studied.
There is no threshold where danger suddenly begins.
There is only a curve.
Clinical cutoffs exist because clinicians need decision points and trials need entry criteria. They are administrative tools. They are not biological truths. The arteries do not know what the cutoffs are.
This is the limitation of categorical thinking in a continuous disease, and it sits beneath the failures described in the rest of this brief.
The 2025 Update
The 2025 guideline did not change the diagnostic categories themselves.
Category | Blood Pressure Reading |
Normal | Less than 120/80 mm Hg |
Elevated | 120 to 129 systolic and less than 80 diastolic |
Stage 1 hypertension | 130 to 139 systolic or 80 to 89 diastolic |
Stage 2 hypertension | 140 or higher systolic, or 90 or higher diastolic |
Table 1. AHA/ACC blood pressure categories (unchanged in the 2025 update).
What changed is how risk is calculated, when treatment is initiated, who is screened for secondary causes, how diagnosis is confirmed, and which therapies are now available. The guideline issued eight major updates spanning risk assessment, secondary cause screening, monitoring practices, treatment initiation, special populations, cognitive prevention, and procedural therapy in resistant cases.
Three of those updates have direct, immediate implications for how care is delivered to the high-performing adults this brief addresses. They are the focus of what follows.
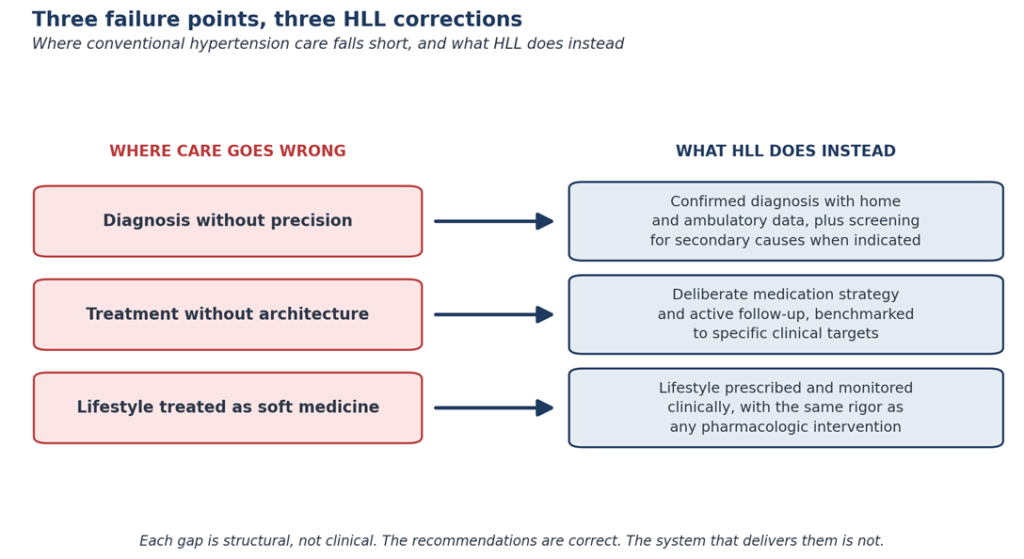
Failure Point One: Diagnosis Without Precision
The simplest failure in hypertension care is the one that happens before treatment is ever discussed. Office blood pressure measurement, performed in the way it is typically performed, is not reliable enough to confirm or exclude the diagnosis on its own.
The 2025 guideline reinforces what hypertension specialists have advocated for years. Diagnosis should not rest on office readings alone. Out-of-office measurement, through home blood pressure monitoring or 24-hour ambulatory monitoring, is needed to confirm the diagnosis, to identify masked hypertension (normal in clinic, elevated outside it), and to identify white-coat hypertension (elevated in clinic, normal outside it). These are not edge cases. Each is common, each carries different prognostic implications, and each requires different management.
Many practices do not have the time, infrastructure, or follow-through to operationalize this. So they do not. Diagnosis is made from a single reading taken in a hallway after the patient has rushed in from the parking lot.
The second diagnostic failure is more consequential and less appreciated.
Primary aldosteronism is a treatable, sometimes surgically curable form of secondary hypertension caused by autonomous overproduction of the hormone aldosterone. It accounts for an estimated 5 to 10 percent of all hypertension cases and up to 20 percent of resistant cases. It carries higher cardiovascular risk than essential hypertension at equivalent blood pressure levels, and it responds to specific therapies that are not first-line for essential hypertension.
It is also screened in fewer than 2 percent of eligible patients in routine clinical care.
The 2025 guideline expanded the screening recommendation to include all patients with stage 2 or resistant hypertension, regardless of potassium level. The rationale is straightforward. The condition is more common than has been clinically appreciated, the screening is inexpensive, and the treatment options are specific and effective.
For the audience of this brief, the practical implication is this. A diagnosis of hypertension based on office readings, treated empirically without screening for the most common identifiable cause, in a setting where home monitoring is not built into the protocol, is a diagnosis that may be incomplete in important ways. Even when the pressure number is real, the underlying mechanism may be missed.
The work of getting this right takes time, infrastructure, and a willingness to look beyond the standard panel. It is also where concierge medicine has structural advantages that fee-for-service primary care cannot match.
Failure Point Two: Treatment Without Architecture
For patients with stage 2 hypertension, defined as 140/90 mm Hg or higher, the 2025 guideline reinforces a recommendation that has been increasingly clear for several years. Initial therapy should usually involve two medications from different classes, ideally combined into a single daily pill, rather than a single agent escalated over months.
The evidence is straightforward. A single medication can only do so much before the body’s compensatory systems blunt its effect. Two medications acting on different pathways are more effective and, perhaps counterintuitively, often better tolerated, because each can be used at a moderate dose rather than a high one.
Single-pill combinations, in randomized trials, improve adherence and shorten time to control compared with separate prescriptions. The reason is simple. Patients are more likely to take one pill than two.
This is precise medicine in the most pragmatic sense. It is not aggressive. It is well-engineered.
The architectural failure in conventional care is not the absence of these medications. The agents themselves are widely available. The failure is in how care is organized around them.
Most patients with newly diagnosed stage 2 hypertension are started on a single agent, told to return in three months, given little support in the interim, and rarely have their progress benchmarked against any specific target. Many never reach control. Some are added to a second agent only after a year of an unsuccessful first.
The 2025 guideline reinforces a model of care that primary care, in the typical fee-for-service structure, is rarely positioned to deliver. Frequent follow-up. Active medication adjustment. Home monitoring data integrated into the decision-making. Patient education that is deep enough to be acted on.
That model is what HealthSpan Longevity Living has been built to deliver.
Failure Point Three: Lifestyle Treated As Soft Medicine
The 2025 guideline gets specific about lifestyle in a way previous guidelines did not. The recommendations are not framed as gentle suggestions. They are framed as clinical prescriptions, with numerical targets, supported by trial-level evidence.
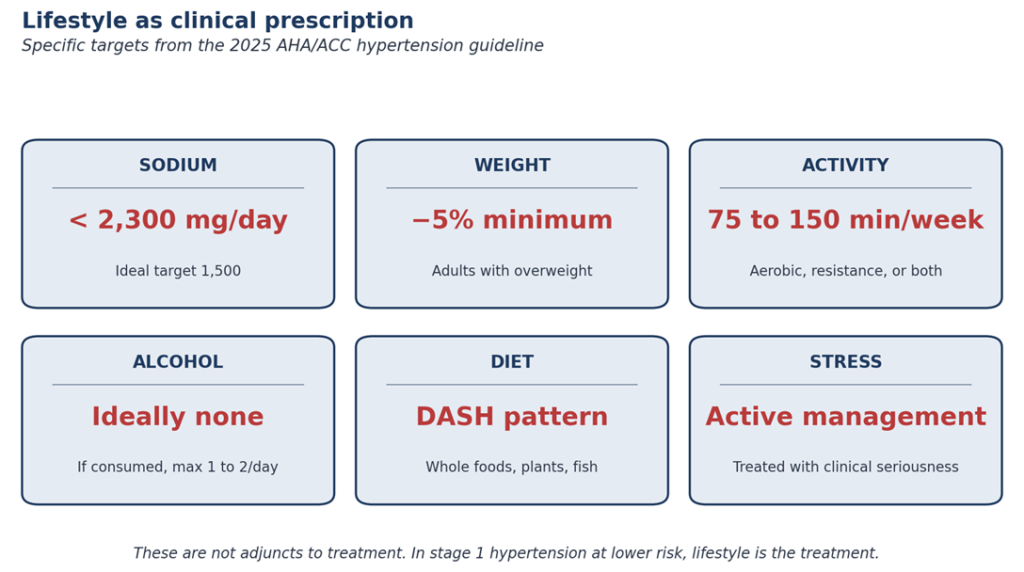
These targets are not adjuncts to other treatment. In stage 1 hypertension at lower cardiovascular risk, lifestyle is the treatment, prescribed for three to six months before pharmacologic therapy is added. In every stage, lifestyle changes alter the medication ultimately required, the side-effect burden carried, and the long-term arterial damage that accumulates.
The reason lifestyle care fails in conventional practice is rarely that the recommendations are wrong. The recommendations are correct, and have been for years. The failure is that the system does not deliver them. A 12-minute appointment cannot teach DASH eating, prescribe an exercise structure, address sleep architecture, screen for and intervene on stress, and follow up on adherence. None of it gets done with the seriousness it deserves.
This is not a failure of the patient. It is a failure of the design.
What the 2025 guideline calls for is what concierge medicine has long been positioned to provide. Time. Specificity. Follow-up. The physician sees the patient often enough to make adjustments before drift becomes deviation.
Lifestyle is not soft medicine.
It is medicine that depends on a system willing to deliver it.
What Healthspan Longevity Living Does Differently
The three failures above are not theoretical. They describe the difference between the care most adults receive and the care that the 2025 guideline describes as appropriate.
HLL is built to close that gap.
Diagnosis at HLL is not a single office reading. It combines office, home, and where appropriate ambulatory measurement, paired with screening for primary aldosteronism and other secondary causes when stage 2 or resistant patterns appear. The work of confirming the diagnosis correctly takes time. The time is built into the model.
Treatment at HLL begins with a deliberate architecture. The right medication classes, at appropriate doses, in single-pill combinations where the evidence supports it, with active follow-up rather than annual review. The goal is not merely an acceptable office number. The goal is sustained, evidence-based risk reduction.
Lifestyle at HLL is treated as clinical. Sodium, potassium, weight, activity, alcohol, sleep, and stress are evaluated, prescribed, and followed up on with the same rigor as any pharmacologic intervention. The patient is not handed a brochure. The work is shared between the physician and the patient over the year, not addressed once and forgotten.
This is not a different philosophy of medicine. It is the application of the medicine that the 2025 guideline already recommends, delivered in a setting designed to actually do it.
Closing
Most adults with hypertension are diagnosed late, treated incompletely, and never receive lifestyle care delivered with the seriousness the evidence requires. The arteries do not forgive this. They respond to the pressure they are under, every day, for as many years as the pressure is there.
The 2025 guideline clarified the standard. Many routine care settings have not yet built the systems required to deliver it consistently.
For the executive reader of this brief, the practical question is simple. Whatever the office reading on the last physical may have shown, the underlying questions are these.
Has the diagnosis been confirmed with the precision the evidence requires?
Is the treatment, if any, organized around current best practice or the practice of a decade ago?
Is the lifestyle prescription being treated as a clinical prescription?
Where the answer to any of these is no, the work is unfinished.
HealthSpan Longevity Living was built for the work of finishing it.
The HLL founding cohort is now opening in Atlanta.
For individuals who want a more precise, prevention-focused approach to cardiovascular risk, information and registration are available at:
healthspanlongevityliving.com/launch-waitlist-2026
DISCLAIMER
This clinical brief is for educational purposes only and does not replace individualized medical advice, diagnosis, or treatment. Blood pressure treatment decisions should be made with a qualified clinician who can evaluate the full clinical context.
REFERENCES
- Jones DW, Ferdinand KC, Taler SJ, et al. 2025 AHA/ACC Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. Journal of the American College of Cardiology. Published online August 14, 2025. doi:10.1016/j.jacc.2025.05.007
- Brown C, Clark D III, Jones DW. Updates in the 2025 AHA/ACC Hypertension Guideline. Current Hypertension Reports. 2026;28(1):19.
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, for the Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903-1913.
- American Heart Association. Heart Disease and Stroke Statistics 2025 Update. Circulation. 2025;151(8):e1-e660.
- Brown JM, Siddiqui M, Calhoun DA, et al. The Unrecognized Prevalence of Primary Aldosteronism: A Cross-sectional Study. Annals of Internal Medicine. 2020;173(1):10-20.
- Neal B, Wu Y, Feng X, et al. Effect of Salt Substitution on Cardiovascular Events and Death (SSaSS). New England Journal of Medicine. 2021;385:1067-1077.
- Parati G, Kjeldsen S, Coca A, Cushman WC, Wang J. Adherence to Single-Pill Versus Free-Equivalent Combination Therapy in Hypertension: A Systematic Review and Meta-Analysis. Hypertension. 2021;77(2):692-705.