
Cardiovascular disease remains the leading cause of death in American adults. The biology that drives it begins decades before the first symptom. By the time chest pain shows up at age 60, the arterial damage has been accumulating since the 30s.
In March 2026, the American College of Cardiology and the American Heart Association, together with nine other societies, released the first comprehensive update to the cholesterol guideline since 2018. The document was renamed. It was restructured. It moved the recommended preventive standard meaningfully forward.
Three changes matter most for the audience HLL serves.
- The risk calculator changed. PREVENT replaces the older Pooled Cohort Equations. Risk assessment now begins at age 30, not 40.
- LDL cholesterol goals are back. The 2018 guideline removed numerical targets. Practice drifted. The 2026 guideline restores them, and they are tighter than what most adults on therapy are currently achieving.
- Lipoprotein(a) screening is now universal. Every adult should have it measured at least once. About 1 in 5 adults have an elevated level. Most never know.
Each of these changes has direct implications for how cardiovascular prevention is delivered. Each is also a place where most routine care has not yet caught up. Each is addressed in turn below.
Table of Contents
The Scope of the Problem
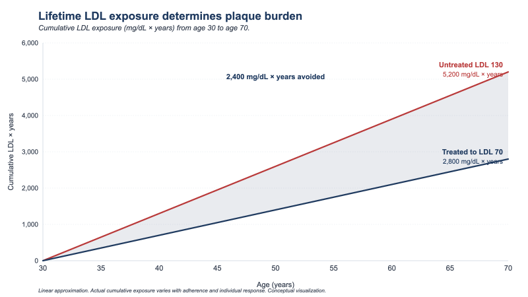
Atherosclerosis is a disease of accumulation. Plaque builds in arterial walls one decade at a time. The body compensates until it cannot. The first event, a heart attack or stroke, is rarely the beginning of the disease. It is the late stage of a process that has been underway for thirty or forty years.
Three statistics anchor the problem.
Roughly 25 percent of American adults have an LDL cholesterol of 130 mg/dL or higher.
Roughly 1 in 250 to 300 adults have a heterozygous familial hypercholesterolemia phenotype, a genetic disorder that produces lifelong elevated LDL.
Most young adults have had lipid values checked, if at all, without a full interpretation of lifetime exposure, family history, inherited risk, and early imaging markers.
The 2018 guideline framed cholesterol management around a risk score. The score determined whether a statin was offered. If risk was below threshold, no treatment. If risk was above threshold, a statin at fixed intensity. Specific LDL targets were removed. The result, predictably, was variability. Some patients reached aggressive lipid levels. Many did not. Few practices systematically followed up to find out.
The biology of cholesterol is not categorical. It is cumulative. Every milligram per deciliter of LDL, present in the bloodstream for every year of adult life, contributes to plaque burden. The relationship is approximately linear and approximately permanent. Lower for longer is better. The 2026 guideline says this explicitly.
The 2026 Update
The 2026 document retired and replaced the 2018 cholesterol guideline. It was renamed from “Blood Cholesterol” to “Dyslipidemia” to reflect that LDL is no longer the only lipid that matters. Triglyceride-rich remnant particles and lipoprotein(a) are now formally part of the assessment.
Three updates drive most of the practical implications for adult prevention. Each is treated below.
Change One: Risk Assessment Moved to PREVENT
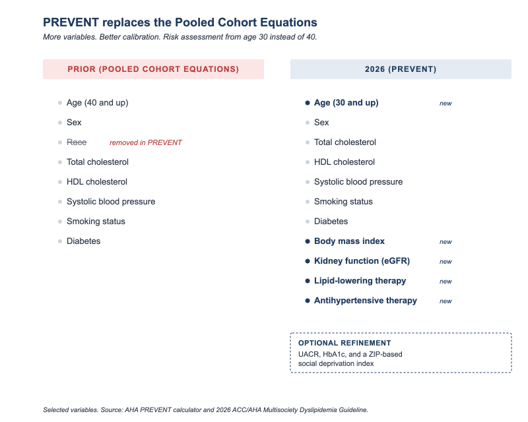
For a decade, U.S. cardiology used the Pooled Cohort Equations to estimate 10-year risk of a heart attack or stroke. The PCE were developed in the early 2010s and validated on data from earlier decades. They were known to be miscalibrated for several populations and to overestimate risk in some groups while underestimating it in others.
PREVENT was developed on more recent and more diverse data. It excludes race as a biological predictor. It incorporates cardiovascular, kidney, and metabolic variables, including age, sex, cholesterol, systolic blood pressure, smoking status, diabetes, body mass index, kidney function, lipid-lowering therapy, and antihypertensive therapy. Optional inputs, including UACR, HbA1c, and a ZIP-code-based social deprivation index, can further personalize the estimate. PREVENT produces both a 10-year and a 30-year risk estimate. It can be used starting at age 30, not 40.
The age threshold matters. Heart disease prevention does not start at 40. Atherosclerosis does not wait for the age thresholds used in clinical trial enrollment. Risk identified at 32 and addressed for the next thirty years has a fundamentally different outcome than risk identified at 52 and partially addressed for ten.
For primary prevention, the 2026 guideline lowers the thresholds at which lipid-lowering therapy enters the conversation. Therapy can be considered at a 10-year PREVENT risk of 3 to 5 percent. It should be considered at 5 to 10 percent. Both numbers sit lower than the prior framework supported in practice.
The guideline also formalizes a three-step process called CPR. Calculate the risk. Personalize it by considering factors PREVENT cannot capture, including family history, lipoprotein(a), and lifestyle. Reclassify when needed using selective coronary artery calcium scoring.
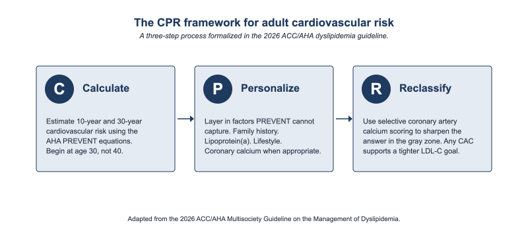
The CAC scan is the single most useful test for sharpening risk in adults the calculator places in the gray zone. Any calcium at all in the coronary arteries indicates established atherosclerosis. Higher amounts indicate more advanced disease. The 2026 guideline supports CAC scoring to refine decisions in men aged 40 and older and women aged 45 and older. Any CAC at all supports an LDL-C goal of less than 100 mg/dL. Substantial CAC supports lower targets still.
Change Two: LDL Cholesterol Goals Are Back
The 2018 guideline removed specific LDL cholesterol goals. The intent was to simplify. The result, in many practices, was that a statin was prescribed and the conversation ended. Whether the patient’s LDL ever reached an evidence-based target was rarely measured and almost never followed up.
The 2026 guideline restores explicit numerical goals for both LDL-C and non-HDL-C. They are anchored to risk. They are tighter than most adults on statins are currently achieving.
Risk Category | LDL-C Goal | Non-HDL-C Goal |
Secondary prevention, very high risk | < 55 mg/dL | < 85 mg/dL |
Secondary prevention, not very high risk | < 70 mg/dL | < 100 mg/dL |
Primary prevention with diabetes plus risk enhancers | < 70 mg/dL | < 100 mg/dL |
Primary prevention with diabetes alone | < 100 mg/dL | < 130 mg/dL |
LDL ≥ 190 mg/dL without familial hypercholesterolemia | < 100 mg/dL | < 130 mg/dL |
Heterozygous familial hypercholesterolemia | < 70 mg/dL | < 100 mg/dL |
Heterozygous FH with established ASCVD | < 55 mg/dL | < 85 mg/dL |
Any coronary artery calcium | < 100 mg/dL | < 130 mg/dL |
Table 1. 2026 LDL-C and non-HDL-C goals across risk categories.
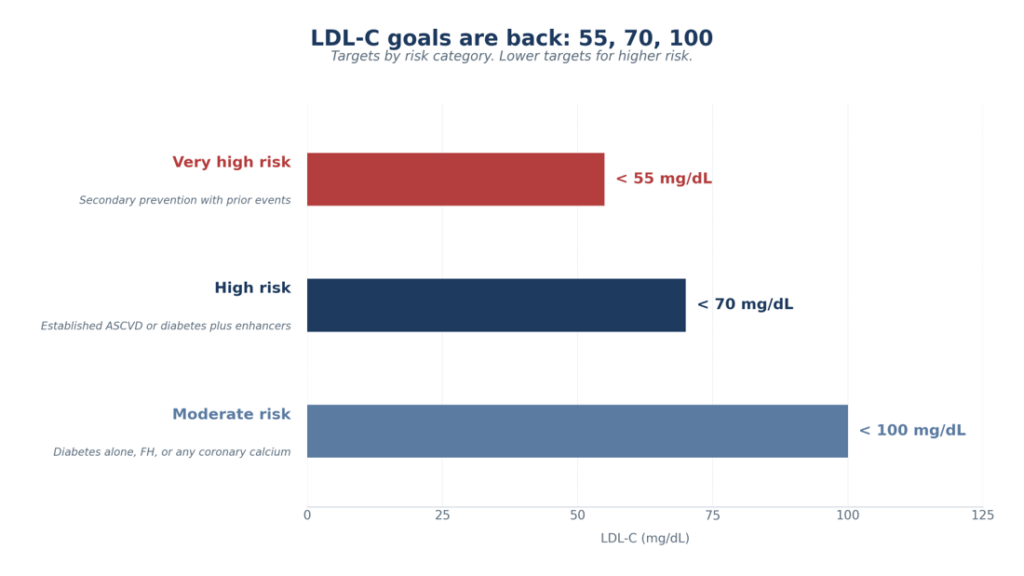
A useful framing comes from the writing committee itself. The targets cluster around three numbers. 55, 70, 100. Highest risk targets 55. Intermediate risk targets 70. Lower risk with at least one major signal targets 100. The number tightens as cumulative risk climbs.
The therapeutic toolkit is meaningfully larger than it was in 2018. Statins remain foundational. Ezetimibe is added when statins alone do not reach goal. Depending on the patient’s risk category, response, tolerance, cost, and access, additional evidence-based options include bempedoic acid and PCSK9 monoclonal antibodies. Inclisiran is also available as a twice-yearly LDL-lowering option, although cardiovascular outcomes data are still being studied. For the rare patient with homozygous familial hypercholesterolemia, the guideline incorporates evinacumab, an ANGPTL3 inhibitor that lowers LDL through a mechanism independent of the LDL receptor.
The relevance for an executive audience is concrete. Most adults on a statin in routine care have not been titrated to a 2026 goal. Statin alone, at modest dose, started without a baseline LDL drawn first, never followed up to confirm the target was reached, is not the standard the evidence now supports. Reaching the goal often requires combination therapy. Combination therapy requires a clinician with the time and infrastructure to use it.
Change Three: Universal Lipoprotein(a) Screening
This is the most consequential change in the document.
Lipoprotein(a), or Lp(a), is a particle in the blood that resembles LDL but is genetically distinct. Levels are roughly 90 percent inherited and remain stable across the adult lifespan. Lp(a) does not respond meaningfully to diet, exercise, or statin therapy. It is not affected by weight loss or by lifestyle change of any kind.
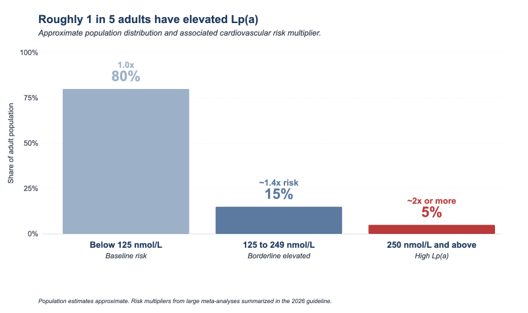
Elevated Lp(a) is one of the most important and one of the most underrecognized cardiovascular risk factors in adult medicine. Roughly 1 in 5 adults globally have an Lp(a) level high enough to substantially raise their risk of heart attack, stroke, and aortic stenosis. Most never know. The standard lipid panel does not include it.
The 2026 guideline recommends, with Class I designation, that every adult have Lp(a) measured at least once. This is the first time a major U.S. guideline has made universal Lp(a) screening the standard.
The thresholds matter.
An Lp(a) of 125 nmol/L or higher (about 50 mg/dL) is associated with roughly a 1.4-fold increase in cardiovascular risk.
An Lp(a) of 250 nmol/L or higher (about 100 mg/dL) is associated with at least a 2-fold increase.
The guideline is direct about what to do with the result. An elevated Lp(a) is a reason to lower LDL cholesterol more aggressively, to address every other modifiable risk factor more decisively, and to monitor for clinical disease earlier and more carefully. Targeted Lp(a)-lowering therapies are in late-stage trials and not yet FDA-approved. The clinical strategy in 2026 is to identify the elevated Lp(a) carrier and reduce everything else around it.
Apolipoprotein B is the second underrecognized biomarker the 2026 guideline elevates. ApoB measures the total number of atherogenic particles in the blood. It is more accurate than LDL-C in patients with elevated triglycerides, diabetes, metabolic syndrome, or apparently low LDL on therapy. The 2026 guideline supports ApoB measurement when the standard panel may not tell the full story.
ApoB is particularly useful when triglycerides are elevated, diabetes or metabolic syndrome is present, LDL-C appears deceptively low, or residual risk remains after LDL-C and non-HDL-C goals have been met.
For the audience of this brief, the practical implication is direct. A standard lipid panel is no longer a complete cardiovascular risk assessment. Without Lp(a) measured at least once, and without ApoB available when the standard panel is ambiguous, the most important piece of the picture may be missing.
What HealthSpan Longevity Living Does Differently
The three changes above describe the gap between the care most adults receive and the care the 2026 guideline says they should receive. HLL is built to close that gap.
Risk assessment at HLL begins with the PREVENT equations applied properly, with attention to the factors PREVENT cannot capture. CAC scoring is offered to adults in the eligible age range when it would meaningfully change the conversation about treatment. The risk is calculated, personalized, and reclassified, not generated from a calculator and forgotten.
LDL cholesterol management at HLL is goal-directed. The target is selected based on the individual’s risk profile. The therapy is escalated, in combination, to reach the target. Statin alone is not the end of the conversation when the goal is not met. Ezetimibe, bempedoic acid, PCSK9 monoclonal antibodies, and, where appropriate, inclisiran are part of the toolkit, not afterthoughts.
Lipoprotein(a) is measured once, in every adult, as part of the baseline assessment. ApoB is measured when the standard panel does not tell the full story. The result of either, when elevated, changes the rest of the plan.
Lipid therapy is not considered complete until the target is documented. HLL repeats lipid testing after medication initiation or dose adjustment, confirms whether the LDL-C and non-HDL-C goals have been reached, and escalates therapy when the result remains above target.
This is not a different philosophy of medicine. It is the application of the medicine the 2026 guideline already recommends, delivered in a setting designed to actually do it.
A 46-year-old executive may have a modest 10-year risk by traditional scoring, but elevated Lp(a), a family history of premature heart disease, and early coronary calcium can move the conversation from reassurance to active prevention. That is the difference between routine lipid screening and modern cardiovascular risk assessment.
THE HLL DYSLIPIDEMIA PROTOCOL
• PREVENT-ASCVD 10-year and 30-year risk calculation
• Standard lipid panel with LDL-C and non-HDL-C
• One-time Lp(a) measurement in every adult
• ApoB when the standard lipid panel may underestimate risk
• CAC scoring when risk is uncertain and imaging would change management
• LDL-C and non-HDL-C targets selected by risk category
• Follow-up testing after medication changes until goal is documented
Closing
The 2026 guideline clarified what modern lipid prevention now requires. Most routine care settings have not yet built the systems to deliver it consistently.
For an executive serious about longevity, the question is no longer simply, “Is my cholesterol high?”
The better questions are these.
Has my risk been calculated with PREVENT?
Has my Lp(a) been measured?
Has ApoB been checked when the standard lipid panel may be incomplete?
If I have coronary calcium, diabetes, familial risk, or established vascular disease, is my LDL-C actually at the correct target?
If the answer to any of these questions is no, the prevention work is unfinished.
HealthSpan Longevity Living was built to finish that work.
The HLL founding cohort is now opening in Atlanta.
For individuals who want a more precise, prevention-focused approach to cardiovascular risk, information and registration are available at:
healthspanlongevityliving.com/launch-waitlist-2026
Disclaimer
This clinical brief is for educational purposes only and does not replace individualized medical advice, diagnosis, or treatment. Lipid management decisions should be made with a qualified clinician who can evaluate the full clinical context.
References
- Blumenthal RS, Morris PB, Gaudino M, et al. 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. Published online March 13, 2026.
- Wiggins BS, Barac A, Benziger CP, Blumenthal RS, Cibotti-Sun M, Moore MM, Morris PB. 2026 Dyslipidemia Guideline-at-a-Glance. J Am Coll Cardiol. Published online March 18, 2026.
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC Guideline on the Management of Blood Cholesterol. J Am Coll Cardiol. 2019;73(24):e285-e350.
- Khan SS, Matsushita K, Sang Y, et al. Development and Validation of the American Heart Association’s PREVENT Equations. Circulation. 2024;149(6):430-449.
- Reyes-Soffer G, Ginsberg HN, Berglund L, et al. Lipoprotein(a): A Genetically Determined, Causal, and Prevalent Risk Factor for Atherosclerotic Cardiovascular Disease. Arterioscler Thromb Vasc Biol. 2022;42(1):e48-e60.