Cancer is one of the central threats to longevity. It shortens life, disrupts families, changes identity, and often appears after years of silent biological change.
For many people, the first sign of cancer is not the beginning of the disease. It is the moment the disease has finally become visible.
At HealthSpan Longevity Living, we believe cancer prevention belongs at the center of any serious longevity plan. A longevity program that does not include a disciplined cancer prevention strategy is incomplete, no matter how thoroughly the rest of the body is mapped.
Cancer prevention is not one test. It is a medical framework. It includes reducing modifiable risk, identifying inherited and acquired vulnerability, completing evidence-based screening, acting on abnormal results, and using new early detection technologies with care rather than hype.
In 2026, the American Cancer Society estimates that the United States will see 2,114,850 new cancer cases and 626,140 cancer deaths. Cancer survival has improved substantially, with five-year relative survival for all cancers combined now reaching about 70 percent for people diagnosed from 2015 through 2021. This is progress. It is also a reminder that the best cancer strategy remains prevention whenever possible, earlier detection when prevention is not possible, and careful long-term risk management over a lifetime.
In This Article
Executive Summary
Cancer prevention should be viewed as a pillar of longevity medicine for four reasons.
First, a large proportion of cancer risk is influenced by modifiable factors. A 2024 American Cancer Society study estimated that about four in 10 cancer cases and about one-half of cancer deaths among U.S. adults age 30 and older were attributable to modifiable risk factors, including cigarette smoking, excess body weight, alcohol consumption, physical inactivity, diet, and infections.
Second, cancer is linked to many of the same biological pathways that drive cardiovascular disease, dementia, diabetes, kidney disease, and frailty. Visceral fat, insulin resistance, chronic inflammation, sleep disruption, tobacco exposure, alcohol use, and physical inactivity do not damage only one organ system. They affect the whole person.
Third, evidence-based cancer screening saves lives when it is done correctly and completed consistently. Screening is designed to find cancer before symptoms appear, and in the case of colorectal cancer, screening can also prevent cancer by identifying precancerous lesions before they become invasive. The CDC emphasizes regular screening for breast, cervical, colorectal, and lung cancers before symptoms appear.
Fourth, new technologies such as multi-cancer early detection blood tests are promising, but they require careful interpretation. Some of these tests are commercially available, but they are not yet FDA-approved for routine population screening, and they should not replace established screening tests.
The HLL approach is neither passive nor reckless. We do not wait for symptoms, but we also do not confuse novelty with certainty. We build a cancer prevention plan that is personal, evidence-based, medically supervised, and continuously updated.
Cancer Often Begins Long Before It Is Diagnosed
Cancer is not a single disease. It is a family of diseases characterized by abnormal cell growth, genetic change, immune escape, invasion, and in some cases metastatic spread. Some cancers evolve slowly over many years. Others behave aggressively and become life-threatening quickly.
This is why cancer prevention has to be more than a yearly reminder to stay up to date. A serious cancer prevention plan asks deeper questions.
- What is this person’s inherited risk?
- What is their metabolic risk?
- What is their inflammatory burden?
- What is their exposure history?
- What screening has been completed?
- What screening has been missed?
- What abnormal results were never followed to completion?
- What emerging tests may be reasonable, and what are their limitations?
At HLL, we treat cancer prevention as a longitudinal medical process. The goal is to reduce risk before cancer forms, detect disease earlier when risk cannot be eliminated, and avoid both complacency and overtesting.

The Modifiable Cancer Risk Conversation
Many cancers are not fully preventable. Genetics, aging, random DNA replication errors, environmental exposures, and chance all play a role. Still, it is medically inaccurate to treat cancer as if it is entirely unpredictable.
The American Cancer Society’s prevention guidance focuses on body weight, physical activity, diet, and alcohol use because these factors are among the most important modifiable determinants of cancer risk for people who do not use tobacco. The ACS recommends maintaining a healthy body weight throughout life, being physically active, following a healthy eating pattern, and avoiding or limiting alcohol.
For HLL, this creates a direct link between cancer prevention and our broader longevity model. Cancer prevention overlaps with vascular health, brain health, metabolic health, kidney health, and functional longevity.
A well-built cancer prevention plan should address at least eight domains.
1. Tobacco exposure: still the dominant preventable cancer risk
Tobacco remains one of the most important cancer prevention issues in medicine. Smoking causes cancer and also interferes with the body’s ability to fight cancer. The CDC states plainly that if a person does not use tobacco, they should not start, and if they do use tobacco, they should quit. Quitting can reduce the risk of cancer and other chronic diseases, regardless of how long someone has smoked.
In a longevity practice, tobacco history should be documented with precision.
- Current or former smoking
- Pack-years
- Time since quitting
- Cigar, pipe, vaping, or smokeless tobacco use
- Secondhand smoke exposure
- Prior cessation attempts
- Readiness to quit
- Eligibility for lung cancer screening
For patients with a meaningful smoking history, the cancer conversation must include lung cancer screening when appropriate, but it should not stop there. Tobacco also increases risk for cancers of the mouth, throat, esophagus, bladder, pancreas, kidney, cervix, stomach, colon, rectum, liver, and acute myeloid leukemia.
Tobacco cessation is not simply a lifestyle suggestion. It is cancer prevention, cardiovascular prevention, pulmonary prevention, and longevity medicine.
2. Alcohol: the cancer risk many health-conscious people underestimate
Alcohol occupies a strange place in modern health culture. It is socially accepted, commercially celebrated, and often minimized in conversations about prevention. Yet the cancer data are clear enough that the U.S. Surgeon General issued a 2025 advisory describing a causal link between alcohol consumption and increased risk of at least seven cancers: breast cancer in women, colorectal cancer, esophageal cancer, liver cancer, mouth cancer, throat cancer, and laryngeal cancer.
The American Cancer Society states that, for cancer prevention, it is best not to drink alcohol. For those who do drink, ACS advises limiting intake to no more than two drinks per day for men and one drink per day for women.
This is an important HLL topic because many successful, educated, health-conscious adults are doing several things right. They exercise, take supplements, monitor labs, and undergo executive physicals. Yet they may still drink wine, cocktails, or spirits several nights per week without realizing that alcohol is not metabolically neutral and not cancer-neutral.
The HLL message should be direct but not moralistic.
Alcohol is not just a liver issue. It is a cancer issue.
For patients who want the most aggressive cancer prevention posture, less alcohol is better, and no alcohol may be the most medically defensible target.
3. Excess body weight, visceral fat, and insulin resistance
The cancer discussion must include metabolic health.
The CDC states that overweight and obesity can cause long-lasting inflammation and higher-than-normal levels of insulin, insulin-like growth factor, and sex hormones, all of which may contribute to cancer development. The risk rises with both the amount of excess weight and the length of time a person carries excess weight.
The National Cancer Institute describes strong evidence linking obesity with multiple cancers, and the ACS states that about one in five cancers is linked to excess body weight, physical inactivity, unhealthy diet, and excess alcohol use.
This is why cancer prevention must be integrated with cardiometabolic prevention. A patient with visceral adiposity, hypertension, high triglycerides, low HDL-C, fatty liver, elevated insulin, elevated glucose, sleep apnea, and inflammation does not have isolated weight risk. That patient has a biological environment that may promote vascular disease, dementia risk, kidney disease, and cancer risk at the same time.
At HLL, body composition matters more than body weight alone. We care about waist circumference and visceral adiposity, lean muscle mass, insulin resistance, fatty liver risk, inflammatory markers when clinically appropriate, sleep apnea risk, exercise capacity, and nutrition quality.
Modern obesity treatment, including GLP-1 based medications when medically appropriate, may become part of a cancer prevention conversation. The goal is not cosmetic weight loss. The goal is lower visceral fat, improved insulin sensitivity, better cardiorespiratory fitness, preservation of muscle, and a lower long-term disease burden.
4. Physical activity: cancer prevention through movement
Exercise is one of the most powerful interventions in longevity medicine. It improves blood pressure, insulin sensitivity, lipids, endothelial function, cardiorespiratory fitness, mood, sleep, muscle mass, and functional independence. It is also part of cancer prevention.
The American Cancer Society recommends that adults engage in 150 to 300 minutes of moderate-intensity physical activity per week, or 75 to 150 minutes of vigorous-intensity activity, or an equivalent combination. ACS notes that reaching or exceeding the upper limit of 300 minutes is optimal.
At HLL, we frame exercise as medicine, but with more precision than move more. A cancer prevention exercise plan should include aerobic conditioning, resistance training, reduction in sedentary time, balance and mobility work in older adults, a plan that fits the person’s real life, and measurement of progress over time.
Exercise helps cancer prevention through several plausible pathways: improved insulin sensitivity, lower visceral fat, reduced inflammation, improved immune function, lower estrogen exposure in some contexts, and improved gastrointestinal motility. The full mechanism varies by cancer type, but the clinical direction is clear.
A sedentary body is not a low-risk body.
5. Nutrition: food patterns matter
Cancer prevention nutrition does not require extremes. The best evidence favors durable eating patterns, not rigid short-term diets.
The ACS recommends a healthy eating pattern that includes nutrient-dense foods in amounts that help maintain a healthy body weight, a variety of vegetables, fiber-rich legumes, whole fruits, and whole grains. The guideline also recommends limiting or avoiding red and processed meat, sugar-sweetened beverages, highly processed foods, and refined grain products.
Processed meat deserves special attention. The International Agency for Research on Cancer classifies processed meat as carcinogenic to humans and red meat as probably carcinogenic to humans, with colorectal cancer as the major concern.
For HLL, the practical message is measured. Nutrition should reduce cardiometabolic risk and cancer risk at the same time. A prevention-focused diet should support healthy weight, glucose control, vascular health, gut health, and adequate protein intake, especially as patients age.
This is especially important when patients are using medications for weight loss. Losing fat while losing muscle is not longevity. Any nutrition plan should preserve lean mass, support resistance training, and avoid malnutrition disguised as success.
6. Infection-related cancers and vaccines
Some cancers are linked to chronic infection. This creates one of the most direct cancer prevention opportunities in medicine.
The CDC states that the HPV vaccine can prevent several kinds of cancer, and the hepatitis B vaccine can help prevent liver cancer. CDC also states that HPV causes about 36,000 cancer cases each year in the United States, and HPV vaccination provides safe, effective, lasting protection against the HPV infections most commonly associated with cancer.
For HLL, this topic matters not only for the patient, but for the family. Many of our patients care about their children and grandchildren. Cancer prevention across a family may include HPV vaccination when age-appropriate, hepatitis B vaccination when indicated, hepatitis C screening and treatment when appropriate, HIV prevention and treatment, cervical cancer screening, and counseling about sexual health without stigma.
A cancer prevention plan should not ignore the cancers that can be reduced through vaccination and infection control.
7. Breast cancer screening, dense breasts, and personalized risk
Breast cancer screening should not be generic.
The USPSTF now recommends biennial screening mammography for women ages 40 to 74 years. The recommendation reflects the importance of beginning regular mammography earlier than previous USPSTF guidance.
But mammography is only one part of the breast cancer prevention conversation. Breast density matters. FDA enforcement of the updated Mammography Quality Standards Act regulations began on September 10, 2024, requiring mammography facilities to comply with breast density notification requirements. Dense breast tissue can make cancer harder to detect on mammography, and it may also be associated with higher breast cancer risk.
At HLL, breast cancer prevention is not reduced to a single mammogram on a fixed schedule. Age-based screening is the foundation, but the full risk picture also depends on family history, breast density, prior biopsy results, and genetic risk assessment when indicated. Menopausal status, hormone therapy history, alcohol use, and body composition all influence risk over time. Supplemental imaging may be appropriate for some patients and unnecessary for others. The decision belongs in a careful conversation, not a checklist.
A normal mammogram is reassuring. It is not the whole risk conversation.
8. Colorectal cancer: prevention, not only early detection
Colorectal cancer screening is one of the clearest examples of prevention in clinical medicine. Colonoscopy can identify and remove precancerous polyps before they become invasive cancer.
The USPSTF recommends colorectal cancer screening for adults ages 45 to 75 years. For adults ages 76 to 85, screening should be individualized based on health status, prior screening, and patient preferences.
Patients often think the choice is simply colonoscopy or no colonoscopy. That is too narrow. A good prevention program should explain available options, including colonoscopy, stool-based testing, and follow-up colonoscopy after abnormal noninvasive tests.
The best test is the one that is appropriate for the patient and actually completed.
For HLL, colorectal cancer prevention does not exist in isolation. Diet quality, alcohol use, obesity, insulin resistance, and physical inactivity all change colon cancer risk over time. Family history, inflammatory bowel disease, and prior polyps determine the appropriate screening interval for a given patient. Adherence to that interval is the part that most often fails.
Missed follow-up is a common failure point in cancer prevention. A concierge longevity model should not only recommend screening. It should help ensure completion.
9. Lung cancer screening: finding disease when cure is still possible
Lung cancer remains one of the most lethal cancers, largely because it is often diagnosed late. Screening is available for selected high-risk patients.
The CDC summarizes the USPSTF recommendation for yearly low-dose CT screening in adults ages 50 to 80 years who have a 20 pack-year or greater smoking history, currently smoke or quit within the past 15 years, and are healthy enough to undergo treatment if cancer is found.
Lung cancer screening is not a substitute for tobacco cessation. It is a second line of defense for patients whose risk remains elevated because of their exposure history.
At HLL, every adult patient should have a smoking history documented accurately. Former smoker is not enough. We need pack-years, quit date, symptoms, prior imaging, occupational exposures, and eligibility for low-dose CT.
10. Cervical cancer and HPV-related disease
Cervical cancer is one of the great success stories of screening and vaccination, but it still occurs, especially when screening is missed or follow-up is incomplete.
The current USPSTF cervical cancer screening recommendation applies to women ages 21 to 65, with screening intervals based on age and test type. The topic is being updated, but the principle remains stable: regular cervical screening and HPV-related prevention are essential.
For HLL, cervical cancer prevention should be addressed in a respectful, systematic way that includes screening history, HPV status when available, vaccination history, prior abnormal Pap or HPV results, follow-up of abnormal findings, immunosuppression risk, and smoking history.
Cervical cancer prevention is not glamorous. It is effective medicine.
11. Prostate cancer: individualized screening, not automatic screening
Prostate cancer screening requires nuance.
The CDC summarizes the USPSTF recommendation that men ages 55 to 69 should make an individual decision about PSA-based screening after discussing potential benefits and harms with their clinician.
This is a particularly important topic for HLL because many male clients want aggressive prevention and early detection. That instinct is understandable. It must be guided by careful counseling.
A high-quality prostate cancer discussion should include age, race and ancestry, family history, prior PSA values, PSA velocity and density when relevant, lower urinary tract symptoms, life expectancy, potential downstream testing, the risk of overdiagnosis and overtreatment, and the use of MRI and biomarkers when clinically appropriate.
The goal is not to ignore prostate cancer. The goal is to screen intelligently, interpret carefully, and avoid both delayed diagnosis and unnecessary harm.
12. Multi-cancer early detection blood tests: promise with restraint
Multi-cancer early detection blood tests are among the most discussed technologies in preventive medicine. They are attractive because many cancers do not have established screening tests, and a single blood draw that could detect multiple cancers earlier would be a major advance.
Excitement is not the same as proof.
The American Cancer Society notes that multi-cancer detection tests, also called MCED tests, look for signs of multiple cancers from one blood sample. ACS also states that these tests are not yet FDA-approved, although some are available.
GRAIL states that its Galleri test has not been cleared or approved by the FDA and is performed in a CLIA-regulated laboratory.
The National Cancer Institute’s Vanguard Study is evaluating multi-cancer detection tests to determine how they may perform in a future randomized controlled trial. This reflects the central question. Can these tests improve outcomes, reduce late-stage cancer, and do more good than harm in real-world screening?
At HLL, the responsible position is clear. MCED tests may be considered for selected patients after informed consent, but they should not replace mammography, colon cancer screening, cervical cancer screening, lung cancer screening when indicated, or other evidence-based strategies.
Patients considering MCED testing should understand the limits.
- A negative result does not rule out cancer.
- A positive result is not a cancer diagnosis.
- Follow-up testing may be needed.
- False positives can lead to anxiety, imaging, procedures, and cost.
- Some cancers may be missed.
- Mortality benefit has not yet been established for routine population use.
- Standard screening must continue.
A premium longevity program should not sell fear. It should provide judgment.
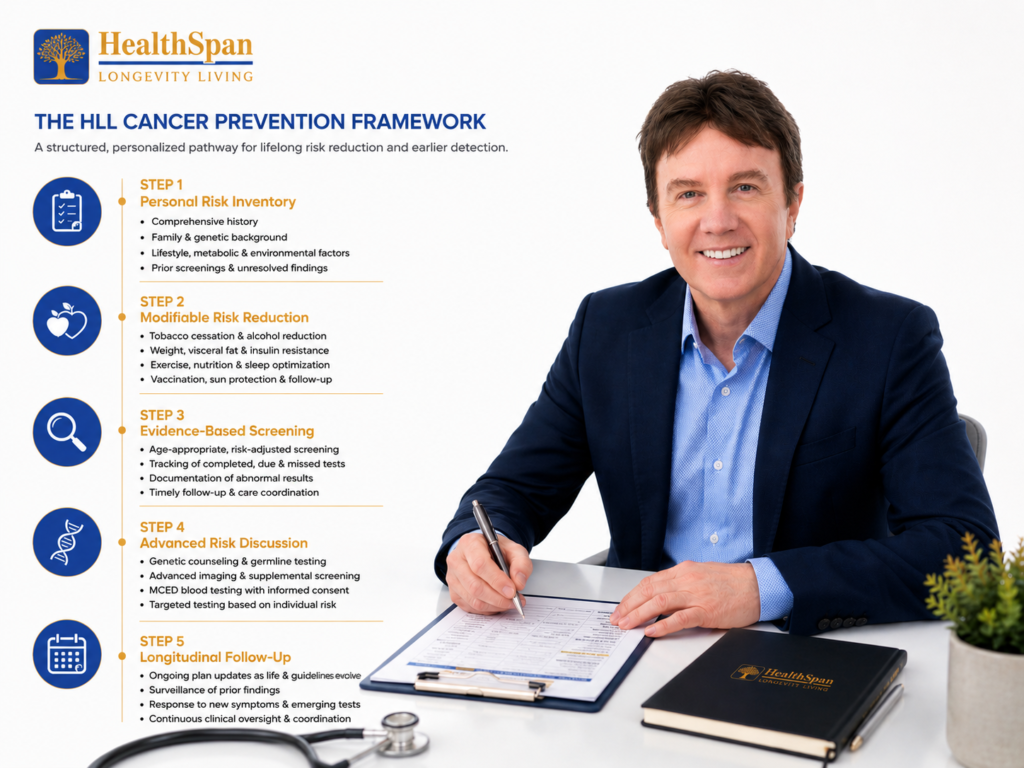
The HLL Cancer Prevention Framework
At HealthSpan Longevity Living, cancer prevention is organized into a structured clinical pathway.
Step 1: Personal risk inventory
We begin with a careful history.
- Age and sex
- Family history of cancer
- Prior cancer or precancerous lesions
- Genetic testing history
- Tobacco history
- Alcohol use
- Body composition and metabolic risk
- Physical activity
- Diet pattern
- Sleep and sleep apnea risk
- Occupational and environmental exposures
- Sun exposure history
- Vaccine history
- Screening history
- Missed follow-up or unresolved abnormal results
Many cancer prevention failures occur because no one has taken the time to build the complete map.
Step 2: Modifiable risk reduction
The prevention plan should address tobacco cessation, alcohol reduction, weight and visceral fat reduction, insulin resistance, exercise prescription, nutrition quality, sleep optimization, vaccination, sun protection, and follow-up of abnormal findings.
This must be individualized. A 42-year-old woman with dense breasts, family history, alcohol use, and insulin resistance needs a different plan from a 68-year-old former smoker with coronary artery disease and a 40 pack-year history.
Step 3: Evidence-based screening
Screening should be age-appropriate, risk-adjusted, and tracked.
A serious program does not merely advise patients to see your doctor for screening. It documents what is due, what has been done, what was abnormal, and what needs follow-up.
Step 4: Advanced risk discussion
Some patients may benefit from additional consideration of genetic counseling, germline testing, breast MRI or supplemental breast imaging, lung cancer screening beyond simple history review, dermatology referral for high-risk skin surveillance, gastroenterology surveillance based on prior polyps, MCED blood testing with informed consent, and targeted imaging when clinically justified.
Advanced does not mean indiscriminate. Better testing is better than more testing.
Step 5: Longitudinal follow-up
Cancer prevention is not a one-day executive physical. It is a living plan.
The plan must be updated as the patient ages, as family history changes, as guidelines evolve, as new symptoms appear, as new tests emerge, and as prior results require surveillance.
This is where HLL distinguishes itself. We do not simply generate data. We interpret it, act on it, and follow it over time.
CANCER PREVENTION AND THE MEANING OF LONGEVITY
Longevity medicine is often marketed through biological age tests, supplements, hormone optimization, and performance metrics. Some of these tools may have a place. The foundation of longevity remains more serious than that.
A person who avoids a preventable cancer gains more than years. They preserve independence, memory, relationships, productivity, and peace. A person whose cancer is detected at an earlier and more treatable stage may avoid the suffering that comes with advanced disease. A family spared a late diagnosis is spared a trauma that statistics cannot fully capture.
This is why cancer prevention belongs in the same conversation as blood pressure, ApoB, coronary calcium, insulin resistance, VO2 max, dementia prevention, and kidney function. These are not separate conversations. They are different windows into the same question.
How do we protect the human being before disease takes command?
HLL POSITION STATEMENT
At HealthSpan Longevity Living, we believe cancer prevention is longevity medicine.
We believe a serious prevention plan should reduce modifiable risk, complete evidence-based screening, identify inherited and acquired vulnerability, use emerging technology responsibly, and follow abnormal findings until there is a clear answer.
We believe early detection should be pursued with intelligence, not fear.
We believe patients deserve more than a generic annual physical and a checklist. They deserve a physician-led strategy that sees the whole person, the whole risk profile, and the long arc of health.
Cancer prevention is not a guarantee. Medicine rarely offers guarantees. It is one of the most meaningful ways to change the trajectory of a life.
The best time to build a cancer prevention plan is before symptoms appear.
That is the work of longevity medicine.
That is the work of HealthSpan Longevity Living.
The HLL founding cohort is now opening in Atlanta.
For individuals who want a more precise, prevention-focused approach to cancer risk, information and registration are available at:
healthspanlongevityliving.com/launch-waitlist-2026
DISCLAIMER
This brief is intended for educational purposes. It does not establish a physician-patient relationship and is not a substitute for individualized medical advice. Recommendations should be reviewed and adapted in the context of a patient’s complete history, examination, and clinical judgment by a qualified physician.
SELECTED REFERENCES
- American Cancer Society. Cancer Facts and Figures 2026. Atlanta: American Cancer Society; 2026.
- American Cancer Society. New ACS study: four in 10 cancer cases and about one-half of cancer deaths in U.S. adults age 30 and older are attributable to modifiable risk factors. Press release, July 11, 2024.
- Centers for Disease Control and Prevention. Cancer Screening Tests. CDC.
- U.S. Department of Health and Human Services, Office of the Surgeon General. Alcohol and Cancer Risk: The U.S. Surgeon General’s Advisory. 2025.
- American Cancer Society. American Cancer Society Guideline for Diet and Physical Activity for Cancer Prevention. CA Cancer J Clin. 2020;70(4):245-271.
- U.S. Food and Drug Administration. Important Information: Final Rule to Amend the Mammography Quality Standards Act. Enforcement of updated MQSA regulations, including breast density notification requirements, began September 10, 2024.
- U.S. Preventive Services Task Force. Breast Cancer: Screening. Recommendation for biennial screening mammography for women ages 40 to 74 years.
- U.S. Preventive Services Task Force. Colorectal Cancer: Screening. Recommendation for adults ages 45 to 75 years, with selective screening for adults ages 76 to 85 years.
- Centers for Disease Control and Prevention. Screening for Lung Cancer. Summary of USPSTF recommendation for yearly low-dose CT in adults ages 50 to 80 with a 20 pack-year or greater smoking history.
- Centers for Disease Control and Prevention. Vaccines and Cancer Prevention. HPV vaccination prevents several cancers; hepatitis B vaccination helps prevent liver cancer.
- American Cancer Society. Multi-cancer Detection Tests. MCED tests look for signs of multiple cancers from a single blood sample, but are not yet FDA-approved, although some are commercially available.
- International Agency for Research on Cancer. IARC Monographs evaluate consumption of red meat and processed meat. Processed meat classified as carcinogenic to humans; red meat classified as probably carcinogenic to humans. [VERIFY against the original IARC monograph before final publication.]