Executive summary
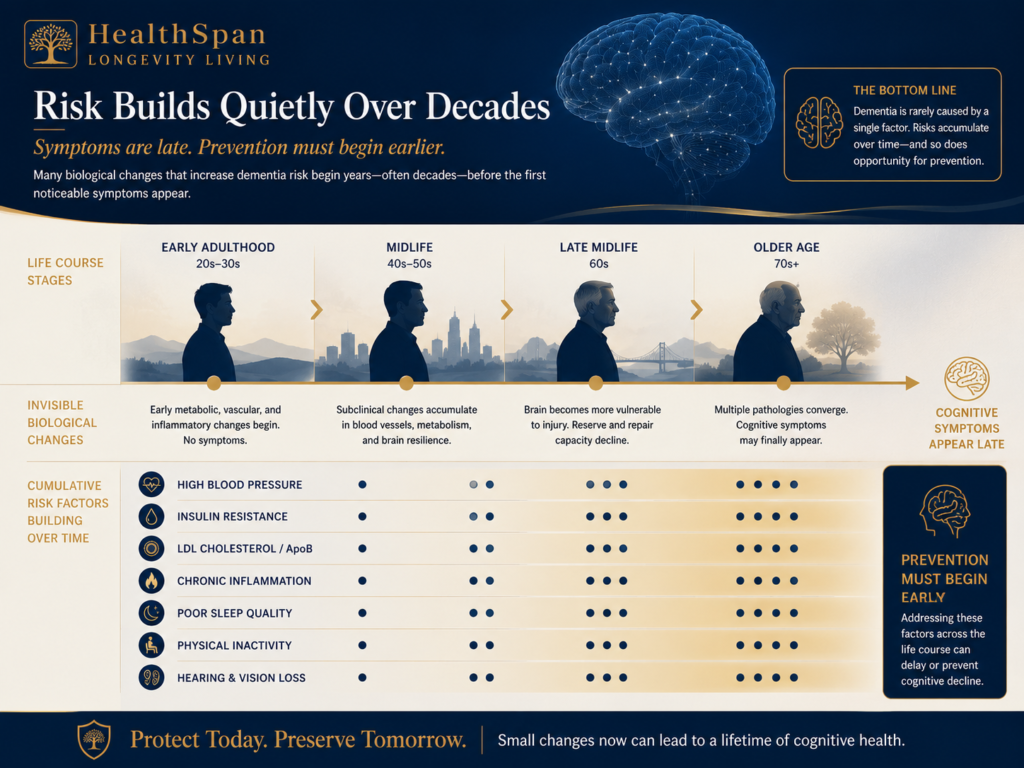
Dementia is usually diagnosed late in life, but the biology that increases risk often begins decades earlier. Long before memory changes are obvious, the brain may already be exposed to elevated blood pressure, insulin resistance, atherogenic lipoproteins, inflammation, poor sleep, reduced fitness, and sensory deprivation.
The most important shift in dementia prevention is not the rejection of the amyloid model. It is the recognition that cognitive decline often reflects several processes occurring at the same time. Alzheimer’s pathology, vascular injury, metabolic dysfunction, sleep disruption, inflammation, and sensory loss can converge on the same patient. That is why prevention cannot be reduced to one drug, one biomarker, or one late-life intervention.
In 2024, the Lancet Commission on dementia prevention, intervention, and care estimated that about 45 percent of dementia cases worldwide may be preventable or delayed by addressing 14 modifiable risk factors across the life course. Two factors were added in the 2024 update: untreated vision loss and elevated midlife LDL cholesterol. Those additions strengthened a point that has direct relevance to cardiovascular medicine: vascular and metabolic risk is brain risk.
This white paper focuses on the cardiovascular, metabolic, and lifestyle drivers of cognitive decline that can be measured, monitored, and treated in a precision prevention model. The goal is not to promise immunity from dementia. No responsible physician can do that. The goal is to identify risk earlier, reduce avoidable injury to the brain, and preserve cognitive function for as long as possible.
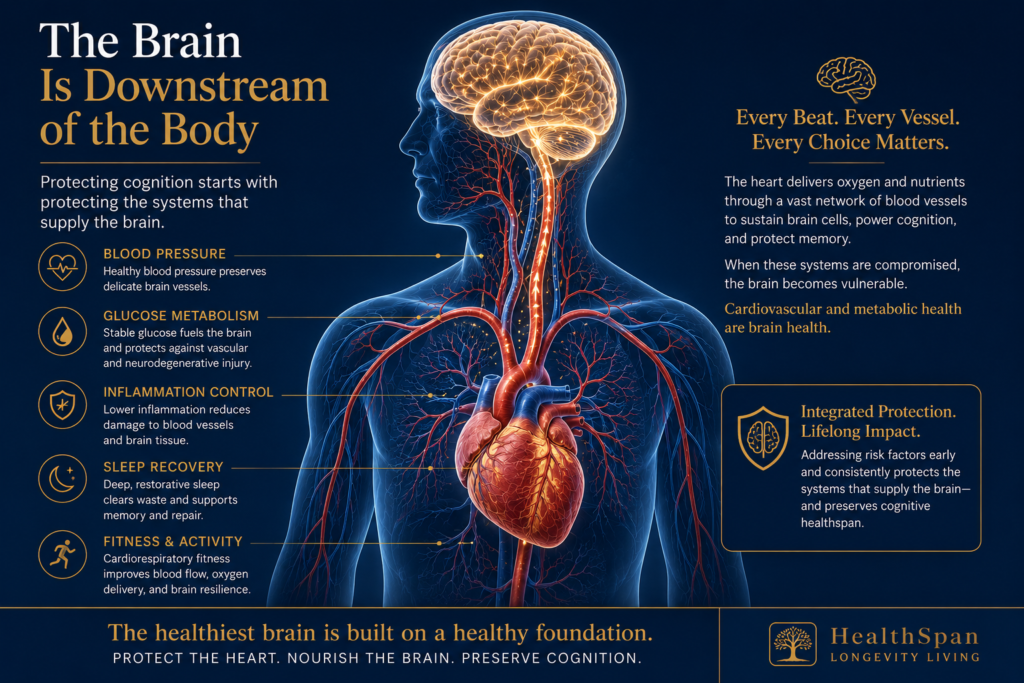
The brain is downstream of the body that supplies it. Protecting cognition begins with protecting the systems that deliver blood, oxygen, and glucose to the brain, support sleep-dependent repair, and maintain metabolic stability.
Core Argument
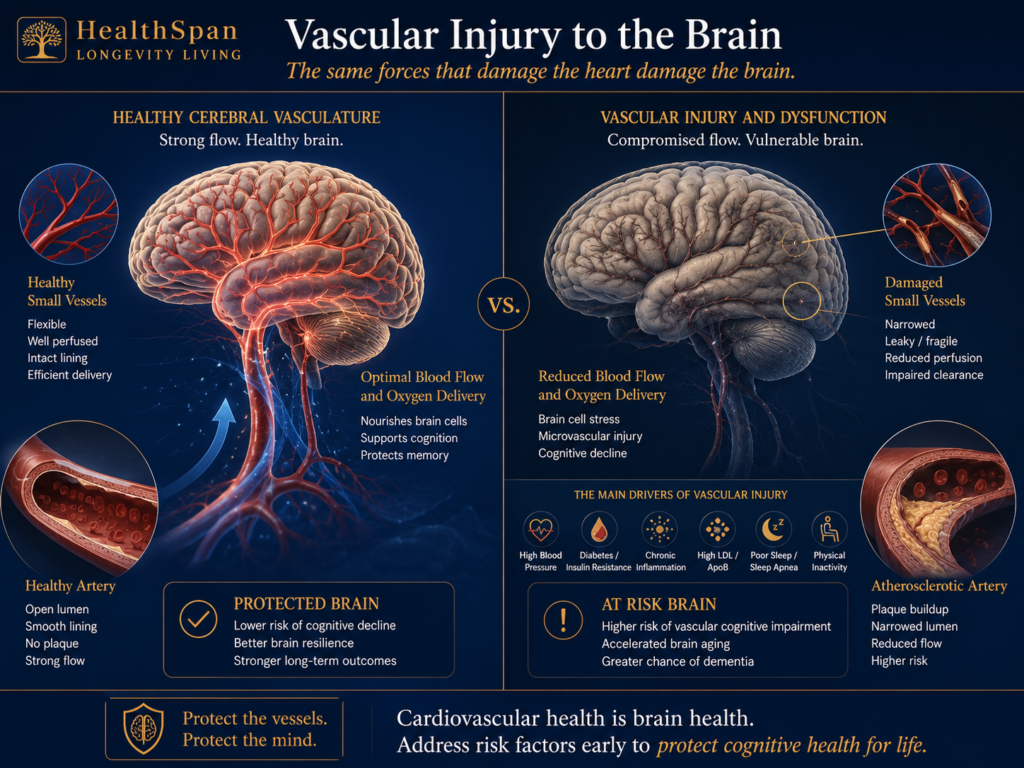
Dementia prevention belongs, in part, within cardiovascular care because the same forces that injure the heart also injure the brain: hypertension, insulin resistance, atherosclerosis, inflammation, impaired sleep, low fitness, and cumulative vascular exposure.
What You'll Find in This Article on Dementia Prevention
A disease process that begins before symptoms
Alzheimer’s disease is the most common cause of dementia, but in older adults it is often not the only process relevant to cognitive decline. Vascular cognitive impairment, cerebral small vessel disease, Lewy body disease, hippocampal sclerosis, neuroinflammation, and mixed pathologies often overlap. In clinical practice, the patient who develops dementia often does not have a single clean mechanism. More often, several vulnerabilities accumulate over time.
For decades, the dominant public narrative of Alzheimer’s disease centered on amyloid plaques. Amyloid remains important. It is central to several approved therapies and to current biomarker definitions of Alzheimer’s disease. But amyloid is not the entire story. Vascular injury, tau pathology, metabolic dysfunction, sleep disruption, inflammation, and genetic susceptibility all influence who develops cognitive impairment, when it appears, and how quickly it progresses.
The timing matters. Biomarker studies show that Alzheimer-related biological changes can begin many years before diagnosis. In one large study, amyloid markers began diverging from cognitively normal controls roughly 18 years before clinical diagnosis, with later changes in tau, neurodegeneration markers, hippocampal volume, and cognition. That does not mean every adult in midlife has Alzheimer’s disease. It means the window for risk modification is much earlier than the first memory complaint.
The clinical question therefore changes. Instead of waiting for cognitive symptoms and then asking what treatment is available, prevention asks a different question: what is happening to the vascular, metabolic, inflammatory, sleep, sensory, and fitness systems that are shaping the brain today?
Stage 0 is where the work happens.
Why cardiovascular care belongs in dementia prevention
The brain weighs only a small fraction of total body mass, but it requires continuous oxygen and glucose delivery. That delivery depends on the heart, large arteries, small vessels, autonomic regulation, endothelial function, and the integrity of the blood-brain barrier. When these systems are injured, the brain becomes more vulnerable to ischemia, inflammation, impaired clearance, and neurodegeneration.
Hypertension and type 2 diabetes are two of the most common drivers of microvascular injury. Both can damage the small vessels of the brain. Both are common for years before they are optimally treated. Both are modifiable. This is why cognitive prevention cannot be separated from cardiovascular prevention.
Vascular contributions to cognitive impairment frequently coexist with Alzheimer’s pathology. Even when the eventual label is Alzheimer’s disease, vascular injury may lower the threshold at which symptoms appear. A patient with amyloid burden and excellent vascular health may follow a different trajectory from a patient with amyloid burden, uncontrolled blood pressure, insulin resistance, sleep apnea, and low fitness.
The brain is not separate from the heart. It is downstream from it.
Blood pressure and the aging brain
Hypertension is one of the strongest modifiable risk factors for cognitive decline. The risk is not confined to severe hypertension. Vascular risk rises across a continuum, and cumulative exposure matters. A blood pressure pattern that looks mildly abnormal at age 45 may carry more long-term brain relevance than a single office reading at age 75.
The Prospective Studies Collaboration, published in The Lancet, showed that vascular mortality risk rises progressively from systolic pressures as low as 115 mm Hg, with stroke and ischemic heart disease mortality roughly doubling for each 20 mm Hg increase in usual systolic blood pressure across a broad adult population. That study was about vascular mortality, not dementia, but the biological lesson is relevant: vascular injury does not begin at a single fixed threshold.
The brain follows the same cumulative logic. Elevated pressure damages penetrating arterioles, contributes to white matter disease, increases the risk of lacunar infarction and microbleeds, and may accelerate the point at which mixed pathology becomes clinically visible. Midlife hypertension appears particularly important because it exposes the brain to injury for years before cognitive decline is recognized.
SPRINT MIND
SPRINT MIND tested whether more intensive systolic blood pressure control could influence cognitive outcomes in hypertensive adults at increased cardiovascular risk. Participants were randomized to an intensive systolic target below 120 mm Hg or a standard target below 140 mm Hg. The trial did not include patients with diabetes or prior stroke, which matters when applying the results to individual patients.
The cognitive results were clinically important. Intensive treatment reduced mild cognitive impairment by about 19 percent and reduced the combined outcome of mild cognitive impairment or probable dementia by about 15 percent. The reduction in probable dementia alone did not reach statistical significance in the original analysis, partly because the parent trial was stopped early after cardiovascular benefit became clear.
Longer follow-up published in 2025 supported the durability of cognitive benefit after the active treatment period. The most responsible interpretation is not that every patient should have the same blood pressure target. It is that careful, sustained blood pressure control is one of the most evidence-based ways to protect both heart and brain, especially when treatment can be achieved safely.
Clinical Implication
Hypertension should not be treated as a number on a chart. It should be treated as cumulative vascular exposure. For cognitive protection, years of control matter more than a single good reading.
Diabetes, insulin resistance, and brain metabolism
Type 2 diabetes is consistently associated with higher dementia risk. The mechanisms include microvascular injury, oxidative stress, inflammation, insulin resistance, impaired blood-brain barrier function, and altered cerebral energy metabolism. Diabetes does not simply raise cardiovascular risk. It changes the metabolic environment in which the brain must function.
Some researchers have used the phrase ‘type 3 diabetes’ to describe insulin resistance within the brain and its relationship to Alzheimer’s pathology. The phrase is useful as a teaching device, but it is not a formal diagnostic category and should not be used as if Alzheimer’s disease and diabetes are the same disease. The more precise point is that metabolic dysfunction and neurodegeneration are biologically linked.
The detection gap is a major clinical problem. Hemoglobin A1c is useful, but it is a delayed marker. Fasting glucose may remain normal while insulin resistance is progressing. In selected patients, fasting insulin, oral glucose tolerance testing, body composition analysis, waist circumference, triglyceride-to-HDL patterns, and continuous glucose monitoring can reveal metabolic drift earlier than routine screening alone.
Visceral adiposity is especially relevant. It contributes to insulin resistance, systemic inflammation, endothelial dysfunction, and cardiometabolic risk. It is therefore a brain variable, not only a weight variable.
A normal fasting glucose is not the same as a healthy metabolism.
Cholesterol, ApoB, Lp(a), and cerebral blood flow
Cholesterol and lipoproteins matter for brain health in two different ways. First, atherogenic particles contribute to plaque formation in the coronary, carotid, and cerebral circulation. Second, lipid handling within the brain is essential to neuronal membrane function, synaptic activity, and repair. Those two realities should not be confused, but both matter.
The 2024 Lancet Commission added elevated midlife LDL cholesterol to its list of modifiable dementia risk factors. The Commission estimated that high midlife LDL cholesterol contributes meaningfully to population-level dementia risk. This does not prove that lipid-lowering therapy alone prevents Alzheimer’s disease. It does support the broader conclusion that midlife lipid exposure is part of cognitive risk assessment.
For cardiovascular prevention, a standard lipid panel is often incomplete. ApoB gives a more direct estimate of the number of atherogenic particles. Lp(a) is largely inherited and is associated with higher risk of myocardial infarction, stroke, peripheral artery disease, and aortic stenosis. The 2026 ACC/AHA multisociety dyslipidemia guideline recommends that every adult have Lp(a) measured at least once in adulthood.
The dementia-specific impact of individual lipid-lowering therapies remains an area of active research. The cardiovascular benefits of statins, ezetimibe, PCSK9 inhibitors, and other lipid-lowering therapies are well established in appropriately selected patients. Protecting cerebral blood flow is part of protecting cognition, even when the cognitive endpoint is harder to prove than the cardiovascular endpoint.
APOE4: genetic risk without fatalism
The APOE4 allele is the strongest common genetic risk factor for late-onset Alzheimer’s disease. One copy increases risk. Two copies increase it further. The presence of APOE4 also has implications for lipid transport, amyloid handling, blood-brain barrier integrity, and treatment risk discussions in selected settings.
APOE4 is not destiny. Many carriers never develop dementia, and many people who develop dementia do not carry APOE4. The value of knowing APOE status, when a patient chooses to know it, is not prediction with certainty. It is the personalization of prevention intensity and counseling.
For APOE4 carriers, the risk management standard should be disciplined. Blood pressure control, metabolic health, fitness, sleep quality, hearing and vision care, alcohol moderation, and lipid assessment become even more important because the margin for error may be narrower.
APOE4 is not a verdict. It is information.
Exercise and cardiorespiratory fitness
Exercise is one of the most consistent modifiable factors associated with lower dementia risk. The strongest signal comes from objective measures of fitness rather than questionnaires. VO2 max is especially useful because it reflects the integrated performance of the heart, lungs, blood, skeletal muscle, mitochondria, and autonomic system.
Fitness protects the brain through several pathways. It lowers blood pressure, improves insulin sensitivity, reduces visceral adiposity, improves endothelial function, and supports cerebral perfusion. Exercise also increases signaling molecules involved in neuronal survival, synaptic plasticity, mitochondrial health, and vascular repair.
Resistance training matters as well. Muscle is a metabolically active tissue. Loss of muscle mass and strength is associated with frailty, insulin resistance, falls, disability, and poorer aging trajectories. Grip strength and muscle function are not vanity metrics. They are clinical signals.
A defensible exercise prescription
- Steady aerobic work at a sustainable intensity, often described as Zone 2, to build mitochondrial capacity and cardiovascular efficiency.
- Higher intensity intervals, when medically appropriate, to improve VO2 max and raise the ceiling of cardiorespiratory fitness.
- Resistance training at least twice weekly to preserve muscle mass, strength, bone density, and metabolic reserve.
The exact protocol should be individualized. The nonnegotiable element is not a perfect workout plan. It is a sufficient and consistent training stimulus across years.
VO2 max is one of the most useful single numbers a person can know about long-term health trajectory.
Sleep and the glymphatic system
Sleep is not idle time. It is active biological maintenance. During sleep, blood pressure regulation, autonomic balance, insulin sensitivity, inflammatory tone, and brain waste clearance are all affected.
The glymphatic system helps move cerebrospinal fluid through brain tissue and supports the clearance of metabolic waste, including beta-amyloid. Deep sleep appears especially important for this process. Chronic sleep restriction, fragmented sleep, untreated sleep apnea, and circadian disruption can therefore affect both cardiovascular and neurological risk.
Short sleep duration is associated with higher risk of cognitive decline, hypertension, metabolic dysfunction, inflammation, and cardiovascular events. The mechanisms overlap. Poor sleep raises nighttime blood pressure, worsens insulin sensitivity, increases sympathetic tone, and can impair recovery after vascular injury.
For most adults, sustained sleep below six hours per night should not be treated as a badge of productivity. It should be treated as a clinical risk signal. APOE4 carriers may be particularly vulnerable to the consequences of poor sleep, although individual risk varies.
Sleep is not a lifestyle footnote. It is a cardiovascular and neurological variable.
Diet and nutrition
The nutrition literature in dementia prevention is less clean than the evidence for blood pressure control, fitness, or smoking cessation. Dietary studies are difficult because adherence is hard to measure, food patterns change over time, and observational data are vulnerable to confounding. Still, a consistent practical signal emerges.
A Mediterranean or MIND-style dietary pattern is the most defensible default. It emphasizes vegetables, leafy greens, legumes, berries, nuts, extra-virgin olive oil, fish, and minimally processed foods, with a lower intake of refined carbohydrates and ultra-processed foods. In a cardiometabolic prevention model, adequate protein must also be protected, especially in older adults who are vulnerable to sarcopenia.
Marine omega-3 fatty acids, particularly EPA and DHA, may support neuronal membrane structure and vascular health. Polyphenol-rich foods, including extra-virgin olive oil, berries, leafy greens, and minimally processed cocoa, may support endothelial and anti-inflammatory pathways. These are not magic foods. They are part of a broader metabolic pattern.
Reducing refined carbohydrates and added sugars can improve insulin sensitivity and reduce visceral adiposity in appropriate patients. In selected patients with mild cognitive impairment, ketogenic dietary patterns are being studied and may have a role, but they should be treated as a clinical tool rather than a population-wide prescription.
Food is not medicine in the casual sense. In a prevention model, nutrition is dose-dependent, measurable, and patient-specific.
Hearing, vision, and sensory health
The 2024 Lancet Commission identified hearing loss and untreated vision loss as important modifiable dementia risk factors. This matters because sensory impairment is common, often undertreated, and clinically addressable.
Hearing loss may contribute to cognitive decline through several pathways. The brain must work harder to decode incomplete auditory input. Social engagement may shrink. Depression and isolation may increase. Over time, the brain that hears less may participate less, and reduced participation is itself harmful.
Vision loss can operate through a similar pathway. Cataracts, diabetic retinopathy, glaucoma, macular degeneration, and uncorrected refractive problems can reduce mobility, reading, exercise, social contact, and environmental stimulation. Some visual problems are treatable, and some are preventable with better cardiometabolic care.
Hearing and vision are not minor quality-of-life issues. They are cognitive health variables.
Inflammation and cumulative risk burden
Chronic systemic inflammation is increasingly recognized as a contributor to vascular disease, metabolic disease, and neurodegenerative risk. The clinical goal is not simply to suppress inflammation in isolation. It is to identify why inflammation is present, then treat the modifiable drivers behind it.
Common contributors include visceral adiposity, insulin resistance, untreated periodontal disease, chronic infections, autoimmune disease, poor sleep, smoking, heavy alcohol use, and sedentary behavior. Inflammatory markers such as high-sensitivity C-reactive protein can be useful in selected patients, but these markers are only starting points. The work is to identify and reduce the biological burden behind the elevation.
The Lancet Commission also includes depression, social isolation, smoking, traumatic brain injury, excessive alcohol use, low education, physical inactivity, obesity, diabetes, hypertension, air pollution, hearing loss, vision loss, and high midlife LDL cholesterol among modifiable risks. No single factor explains dementia. The aggregate burden is what matters.
Risk that has not been named cannot be managed. Risk that has not been measured cannot be changed.
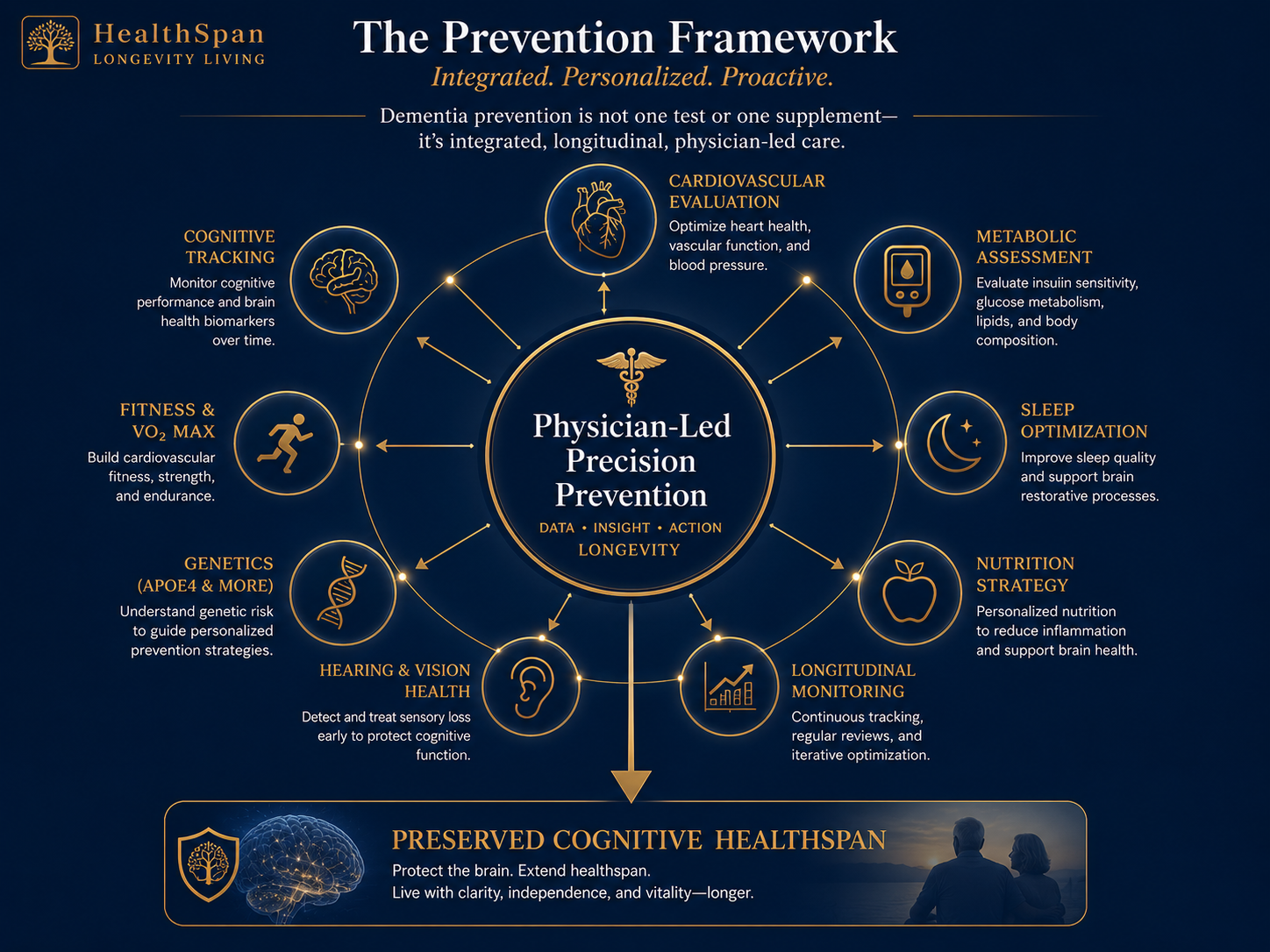
The HealthSpan Longevity Living prevention framework
Dementia prevention in practice does not look like a single test or a single supplement protocol. It looks like a coordinated, longitudinal evaluation of the systems that influence cognitive risk, followed by treatment, measurement, and adjustment over time.
At HealthSpan Longevity Living, the prevention framework is built around physician-led integration. The purpose is not to collect data for its own sake. The purpose is to turn data into decisions.
Cardiovascular evaluation
Blood pressure patterns, lipid burden, ApoB, Lp(a), coronary calcium scoring, and selected imaging can reveal risk long before symptoms or events occur. Coronary and carotid disease are not isolated problems. Atherosclerosis is systemic, and vascular health is part of cognitive health.
Metabolic evaluation
Fasting glucose and hemoglobin A1c are only the beginning. Fasting insulin, oral glucose tolerance testing, body composition, waist circumference, triglyceride patterns, and selected continuous glucose monitoring can identify insulin resistance earlier and more precisely.
Cognitive baseline and tracking
Validated cognitive assessment establishes a baseline. Repeated measurement matters because the most useful signal may be a change relative to the patient’s own prior performance rather than comparison with broad population norms.
Genetic risk assessment
APOE genotyping may be appropriate for selected patients who want the information and understand its implications. It should be paired with counseling. The purpose is to personalize prevention, not to create fear.
Fitness, sleep, and sensory evaluation
VO2 max, muscle strength, sleep quality, sleep apnea risk, hearing, vision, stress, and social engagement are evaluated as clinical variables. These are not soft lifestyle issues. They are measurable determinants of function.
Blood biomarkers
Blood-based biomarkers such as p-tau217, amyloid ratios, GFAP, and neurofilament light chain are advancing rapidly. In 2025, the FDA cleared the first blood test to aid in diagnosing Alzheimer’s disease in symptomatic adults aged 55 and older. These tests should be used carefully, with appropriate counseling and attention to their intended clinical context. Their role in routine prevention for asymptomatic patients remains evolving.
Integration Principle
Tests without integration are data. Data without action is noise. The value comes from physician interpretation, prioritization, treatment, and follow-up.
A practical prevention checklist
For a patient in midlife or early older adulthood, a serious dementia-prevention strategy should usually include the following domains:
- Precise blood pressure measurement and sustained control over time.
- ApoB, Lp(a), and full cardiometabolic risk assessment, not only a basic lipid panel.
- Early detection of insulin resistance using more than fasting glucose alone when risk is present.
- Objective fitness assessment, ideally including VO2 max or a validated proxy.
- Resistance training and preservation of muscle mass.
- Sleep assessment, including screening for obstructive sleep apnea when appropriate.
- Hearing and vision screening with treatment when deficits are present.
- Nutrition designed around metabolic health, adequate protein, and low inflammatory burden.
- Depression, loneliness, alcohol use, smoking, and head injury risk addressed directly.
- Longitudinal tracking so the plan improves as more information accumulates.
What this means in practice
Dementia prevention is not dementia-proofing. It is risk reduction. It is earlier detection. It is the disciplined management of the vascular, metabolic, inflammatory, sleep, sensory, and fitness systems that shape the aging brain.
The evidence is strong enough to act. The 2024 Lancet Commission estimates that about 45 percent of dementia cases may be preventable or delayed, but this is not a guarantee for any individual person. It is a public health signal and a clinical opportunity.
The work is not dramatic in a single visit. It compounds. Better blood pressure control, better metabolic health, better sleep, better fitness, better hearing and vision, lower inflammatory burden, and more deliberate follow-up can change a patient’s trajectory long before symptoms appear.
The cost of doing this work in midlife is mostly attention, measurement, and disciplined care. The cost of not doing it may be paid later by the patient, the family, the business, and the people who depend on that person’s presence and judgment.
The brain is downstream of everything else. Protecting it begins with the body that supplies it.
That is the promise of medicine done carefully over time.
For patients and families
If you are concerned about cognitive decline, family history, cardiovascular risk, diabetes, insulin resistance, APOE4 status, or the long-term preservation of mental performance, HealthSpan Longevity Living provides physician-led evaluation and longitudinal prevention planning for adults who want a deeper relationship than an annual snapshot.
The goal is not more testing. The goal is a coherent plan.

About the author
Dr. Darrel Collins is the founder of HealthSpan Longevity Living, a physician-led precision prevention practice based in Atlanta. He is board certified in internal medicine and cardiovascular disease. His longevity practice extends the work of cardiovascular prevention into the systems that drive cognitive, metabolic, and functional decline, with continuous physician engagement and evidence-based care.
About HealthSpan Longevity Living
HealthSpan Longevity Living is a precision prevention practice for executives, founders, and high-net-worth adults who want a physician relationship rather than an annual snapshot. The practice combines advanced cardiovascular and metabolic evaluation with longitudinal tracking, direct physician access, and an integrated plan that follows the patient across the year, not only across a visit.
Medical note
This white paper is for educational purposes only and does not create a physician-patient relationship. It is not personal medical advice. Clinical decisions should be made with a qualified physician who knows the patient’s medical history, medications, goals, risks, and preferences.
Selected references
- Livingston G, Huntley J, Liu KY, et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet. 2024;404(10452):572-628. doi:10.1016/S0140-6736(24)01296-0.
- Williamson JD, Pajewski NM, Auchus AP, et al. Effect of intensive vs standard blood pressure control on probable dementia: a randomized clinical trial. JAMA. 2019;321(6):553-561. doi:10.1001/jama.2018.21442.
- Reboussin DM, Gaussoin SA, Pajewski NM, et al. Long-term effect of intensive vs standard blood pressure control on mild cognitive impairment and probable dementia in SPRINT. Neurology. 2025;104(3):e213334. doi:10.1212/WNL.0000000000213334.
- Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903-1913. doi:10.1016/S0140-6736(02)11911-8.
- Jia J, Ning Y, Chen M, et al. Biomarker changes during 20 years preceding Alzheimer’s disease. N Engl J Med. 2024;390:712-722. doi:10.1056/NEJMoa2310168.
- Blumenthal RS, Morris PB, Gaudino M, et al. 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of dyslipidemia. Circulation. 2026. doi:10.1161/CIR.0000000000001423.
- S. Food and Drug Administration. FDA clears first blood test used in diagnosing Alzheimer’s disease. May 16, 2025.
- Isaacson RS, Ganzer CA, Hristov H, et al. The clinical practice of risk reduction for Alzheimer’s disease: a precision medicine approach. Alzheimers Dement. 2018;14(12):1663-1673. doi:10.1016/j.jalz.2018.08.004.
- Biessels GJ, Despa F. Cognitive decline and dementia in diabetes mellitus: mechanisms and clinical implications. Nat Rev Endocrinol. 2018;14(10):591-604. doi:10.1038/s41574-018-0048-7.
- Horder H, Johansson L, Guo X, et al. Midlife cardiovascular fitness and dementia: a 44-year longitudinal population study in women. Neurology. 2018;90(15):e1298-e1305. doi:10.1212/WNL.0000000000005290.
- Morris MC, Tangney CC, Wang Y, Sacks FM, Bennett DA, Aggarwal NT. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimers Dement. 2015;11(9):1007-1014. doi:10.1016/j.jalz.2014.11.009.
- Morris MC, Tangney CC, Wang Y, et al. MIND diet slows cognitive decline with aging. Alzheimers Dement. 2015;11(9):1015-1022. doi:10.1016/j.jalz.2015.04.011.
- Barnes LL, Dhana K, Liu X, et al. Trial of the MIND diet for prevention of cognitive decline in older persons. N Engl J Med. 2023;389:602-611. doi:10.1056/NEJMoa2302368.
- Lin FR, Pike JR, Albert MS, et al. Hearing intervention versus health education control to reduce cognitive decline in older adults with hearing loss in the USA: the ACHIEVE randomized controlled trial. Lancet. 2023;402(10404):786-797. doi:10.1016/S0140-6736(23)01406-X.
- Lee CS, Gibbons LE, Lee AY, et al. Association between cataract extraction and development of dementia. JAMA Intern Med. 2022;182(2):134-141. doi:10.1001/jamainternmed.2021.6990.
- Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373-377. doi:10.1126/science.1241224.
- Zare F, Shakhmurova G, Rizaev J, et al. Sleep-dependent clearance of brain metabolites via the glymphatic system: implications for Alzheimer’s pathophysiology. Brain Behav. 2026;16:e71374. doi:10.1002/brb3.71374.